Problem Gambling Prevalence in the UK: PGSI Scores, NHS Surveys and the 18-24 Risk Band
Why the number you hear is almost never the number you need
Every six months, a headline lands. «Problem gambling rates double». «UK problem gambling at record high». «Gambling addiction at lowest level in decade». Half the time the headlines disagree with each other across the same week, and the reason is that they’re quoting different surveys, with different questions, different methodologies, and different definitions of what counts as a problem. Until you understand which number a headline is using, the headline is noise.
I’m a working NBA bettor who has spent the better part of a decade reading these surveys properly, because the gap between «you bet on NBA» and «you have a gambling problem» is a gradient, not a binary, and the regulatory framework around UK gambling is being rebuilt on the assumption that the gradient matters. Anyone who wagers seriously needs to know where on the gradient they sit, and the only way to know is to understand the measurement tools the people writing the rules are using.
PGSI: the scale every UK headline secretly references
The Problem Gambling Severity Index – PGSI – is the dominant tool for measuring at-risk and problem gambling behaviours in Great Britain. It’s a nine-item screening questionnaire developed in Canada in the late 1990s, validated across multiple jurisdictions, and adopted by the Gambling Commission as the standard reference measure for industry surveys.
The questionnaire asks about behaviours over the past 12 months. Each item scores 0 to 3 – never, sometimes, most of the time, almost always – producing a total between 0 and 27. The Gambling Commission groups respondents into four bands based on that total: 0 indicates non-problem gambling, 1 to 2 indicates low-risk gambling, 3 to 7 indicates moderate-risk gambling, and 8 to 27 indicates problem gambling. The headline rate that journalists usually quote is the percentage of adults scoring 8 or higher, which the Gambling Commission and NHS both treat as the clinical threshold for problem gambling.
The nine PGSI items ask about: betting more than you could afford, needing to gamble with larger amounts for the same excitement, returning another day to win back losses, borrowing or selling to fund gambling, feeling you might have a problem, gambling causing health problems including stress and anxiety, criticism from others about your gambling, gambling causing financial problems for you or your household, and feelings of guilt about gambling. The questions are designed to capture the behavioural patterns that distinguish problem gambling from heavy but functional engagement, and the cumulative score reflects severity rather than presence of any single behaviour.
The reason this matters for an NBA punter is that the PGSI gives you a self-administrable diagnostic. You can score yourself honestly against the nine items and know, in objective terms calibrated against population norms, where you sit on the risk gradient. Most engaged punters score in the 0 to 2 zone. A subset score in the 3 to 7 moderate-risk zone, which is the band the regulator has been most focused on shrinking. The 8-plus problem-gambling zone affects a small percentage of the adult population – but the population effect of that small percentage, multiplied across the UK punter base, is what drives policy.
What the NHS prevalence numbers actually show
The two most-cited prevalence sources diverge on the headline number, and the divergence is real, not measurement error.
The NHS Health Survey for England 2024 reported that around 5 percent of adults in England exhibit at-risk or problem-gambling behaviours, with under 1 percent scoring at the clinical problem-gambling threshold. That 5 percent figure aggregates the low-risk, moderate-risk, and problem categories from PGSI scoring – it’s the broad shape of the at-risk gradient, not the narrow clinical threshold.
The Adult Psychiatric Morbidity Survey, jointly published by NHS England and the Department of Health and Social Care, gave a much lower headline number: only 0.3 percent of adults in England met the clinical threshold for problem gambling. The gap between the two surveys reflects methodological differences – the APMS uses a stricter interview methodology applied to a clinical sample, while the Health Survey uses a population-level screening questionnaire with broader inclusion criteria.
Both numbers are correct for what they measure. The 0.3 percent APMS number is the share of adults who, in the formal clinical sense, would be diagnosed with a gambling disorder. The 5 percent Health Survey number is the share of adults exhibiting any at-risk behaviour on the PGSI gradient. The headlines tend to use whichever number suits the editorial line – a lobbying piece favours one, a regulatory-reform piece favours the other. Neither is wrong. They’re answering different questions.
What the data converges on is that the absolute number of UK adults at any non-zero point on the risk gradient is substantial, even if the formal-diagnosis cohort is small. Treatment referrals reflect this. Nearly 2,000 people were referred to specialist NHS gambling services between April and September 2024, up from around 800 across the same six-month window in 2023. That increase reflects both genuine growth in need and reduced friction in the pathway since the NHS took on formal administration of the Gambling Harms Levy in April 2025. The trend is sharply rising.
The 18-24 risk band that should worry the industry
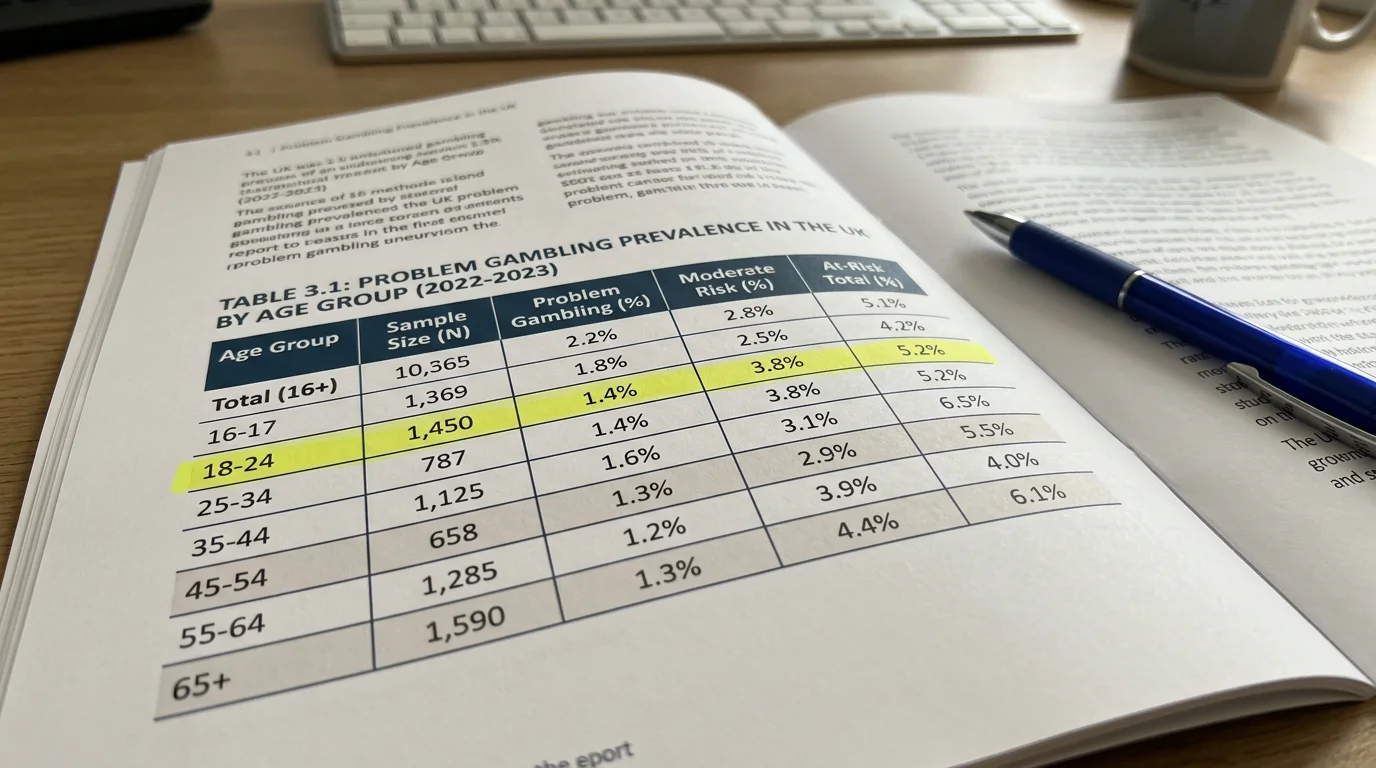
The most striking demographic finding across UK gambling prevalence data is the concentration of risk in young adults. According to Gambling Commission data summarised through Statista, 21.9 percent of British adults aged 18 to 24 score between 1 and 27 on the PGSI scale – meaning more than one in five young adults exhibits at least some at-risk gambling behaviour, the highest rate of any age band by a substantial margin.
That figure is not the problem-gambling rate. It’s the at-risk-gradient rate. But the proportion of 18-to-24-year-olds at any non-zero PGSI score is roughly four times the equivalent rate in the over-55 cohort, and the gap is structural rather than cyclical. The 25-to-34 band is the most active in non-lottery gambling overall in the UK, with around 35 percent participation in late 2025, but the at-risk concentration is heaviest in the immediately younger cohort.
The drivers are debated but broadly converge on a small number of factors. Online gambling availability normalises the activity for a generation that grew up with smartphones, in a way that retail-only access never did for older cohorts. Marketing exposure through sports media – particularly football and increasingly basketball – embeds gambling content alongside fan content during exactly the years that personal habits are forming. The Gambling Commission’s own analysis flags that a person with a problem-gambling profile receives free-bet offers nine times more often than the average customer, which suggests targeting algorithms are reinforcing exactly the risk gradient the regulator is trying to reduce.
Heather Wardle, the public-health researcher whose work informs much of the current policy debate, has been clear about how to read the 18-24 band: «it’s hard to prove what harm is being done because it’s a generational thing and the harm comes much further down the line. We’re creating the conditions that normalise gambling for a generation.» That framing – the harms as cumulative across a life course, not visible in any single year – is the lens the next regulatory wave is being built around.
Referral trends 2024-2025 and what they signal
The most recent NHS data on specialist gambling-harm referrals tells a story the headline prevalence numbers don’t.
Between April and September 2024, nearly 2,000 people were referred to specialist NHS gambling services. The same six-month window in 2023 saw around 800 referrals. The increase is 150 percent year on year. From April 2025, the NHS formally took on administration of the prevention, treatment, and research strands funded by the new statutory Gambling Harms Levy, which substantially expanded the resourcing of the specialist clinic network and reduced the friction in the referral pathway.
Three things explain the increase. The first is supply-side: more clinics, easier referral routes, more GPs and hospital services able to spot the signs and route patients accordingly. The second is genuine demand: the underlying population of people needing help has grown, particularly among the younger demographics where the at-risk gradient is steepest. The third is destigmatisation: the public profile of gambling harm as a treatable health issue, rather than a moral failing, has risen sharply since 2020, and more people are willing to seek help than would have been a decade ago.
The structural funding shift since April 2025 – the levy now sits at a statutory rate paid by every regulated operator, with NHS England administering the spend on a clinical basis – represents the biggest change to the UK gambling-harm treatment infrastructure since the Gambling Act 2005. The direction of travel is toward more clinics, more referral capacity, and a treatment system better integrated into mainstream NHS pathways. For UK NBA punters, the practical consequence is that the help is more accessible than it has ever been if you decide you need it – and the tools that exist before you reach that point, including GAMSTOP and deposit limits, are also more visible across the regulated operator base. The bridge from prevalence data to the practical toolkit lives in my piece on responsible gambling tools at UK NBA bookmakers.
What PGSI score signals problem gambling versus at-risk in NHS reporting?
The PGSI scale runs from 0 to 27, with the Gambling Commission grouping respondents into four bands. A score of 0 indicates non-problem gambling. 1 to 2 indicates low-risk gambling. 3 to 7 indicates moderate-risk gambling. 8 to 27 is the problem-gambling band, which the NHS and Gambling Commission both treat as the clinical threshold. Different headline figures across UK media usually reflect different cuts of the same scale – the broader at-risk figure of around 5 percent captures everyone scoring 1 or higher, while the clinical-threshold figure of around 0.3 percent applies the strict diagnostic standard.
Why has the 18-24 age band the highest at-risk share in UK gambling surveys?
Gambling Commission data shows 21.9 percent of British 18-to-24-year-olds score between 1 and 27 on the PGSI scale, meaning more than one in five young adults exhibits at least some at-risk gambling behaviour. The likely drivers are the normalisation of online gambling for a generation that grew up with smartphones, embedded marketing exposure through sports media including football and increasingly basketball, and targeting algorithms that direct bonus offers heavily toward customers showing early at-risk behaviours. The cohort gap relative to over-55s is roughly four-to-one.
Creado por la redacción de «nba bet of the day».